
INGUINAL HERNIA SURGERY - Dr. BRUTO RANDONE
Dr. Bruto Randone performs Inguinal Hernia Surgery.
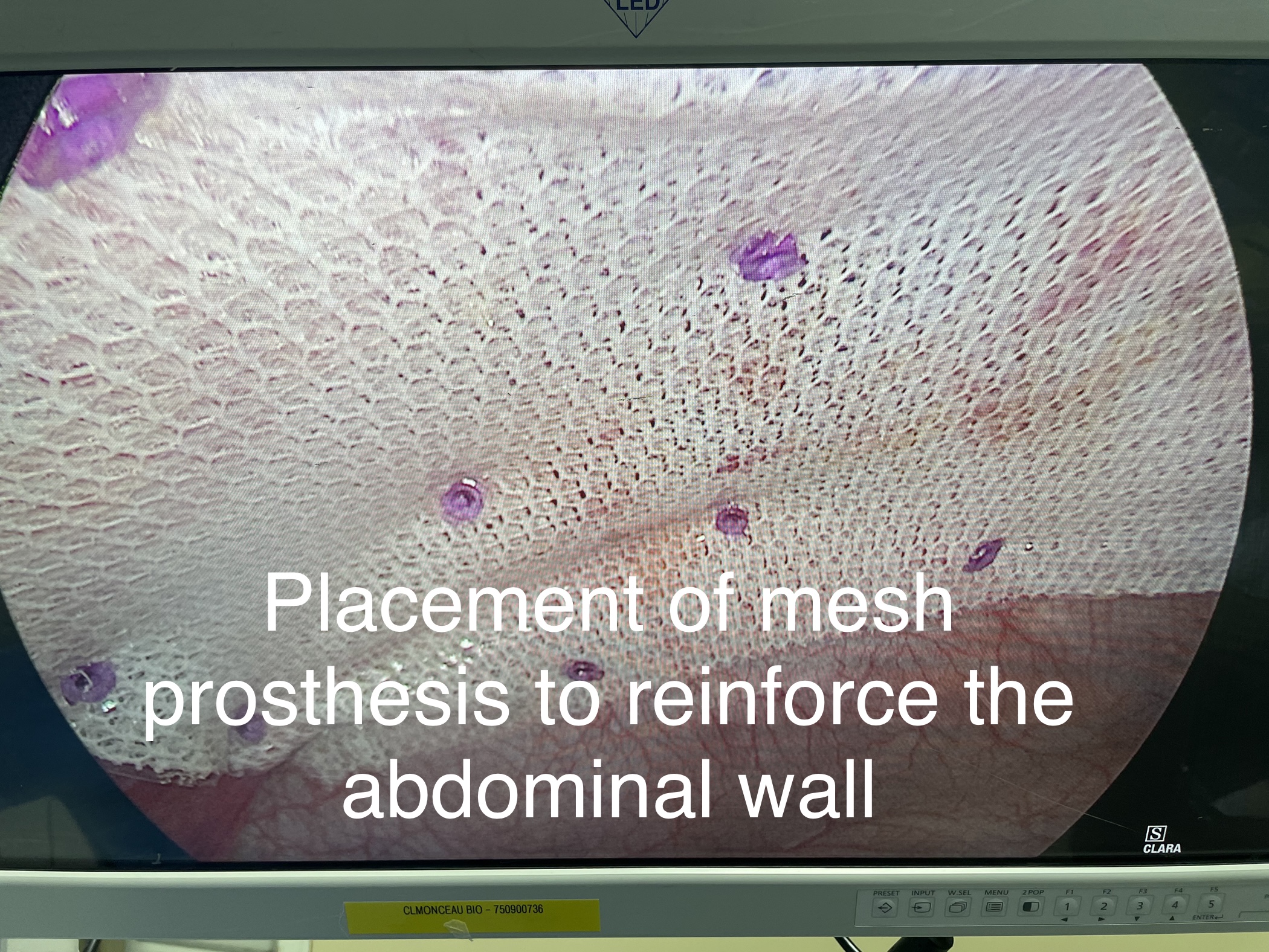
Hernia surgery (inguinal, umbilical) and incisional (generally postoperative) has greatly benefited from laparoscopy, as this method makes it possible to strengthen the weakened wall by placing a MESH REINFORCEMENT PLATE inside the hernia instead of placing it outside. We can see that the plate, placed laparoscopically, rests on the inside of the abdominal wall and therefore the stronger the pressure the more the plate will be pressed against the wall.
Click : LEARN MORE ABOUT PROSTHESES - WHICH PROSTHESIS TO CHOOSE
After surgery
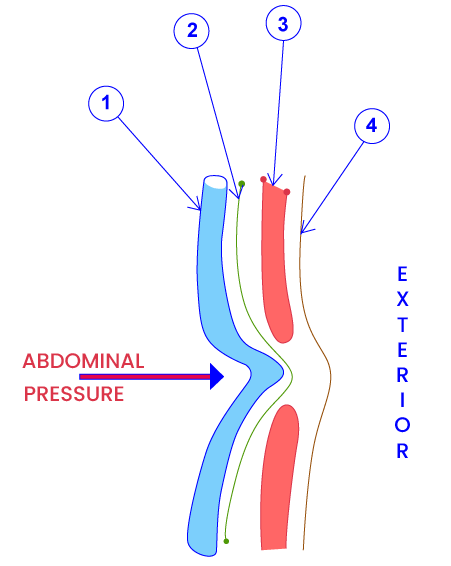
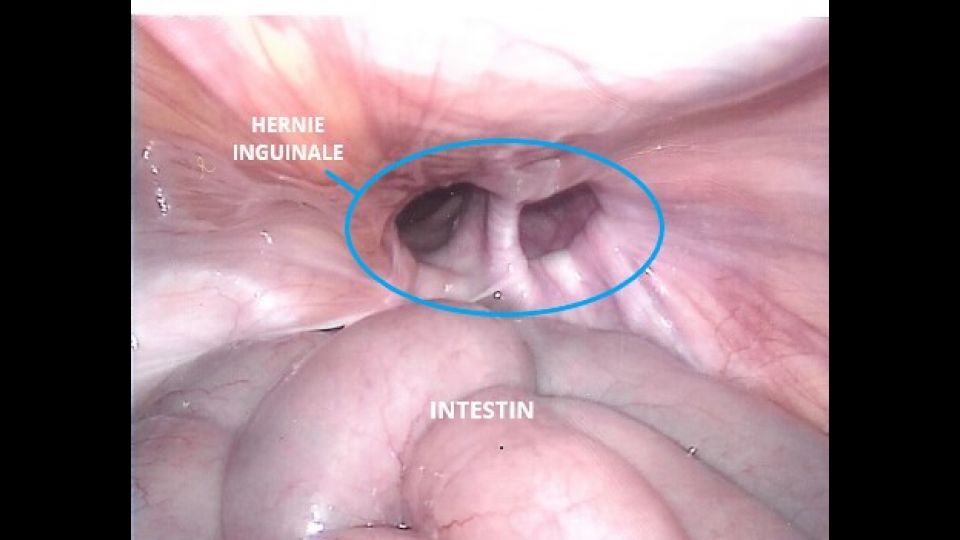
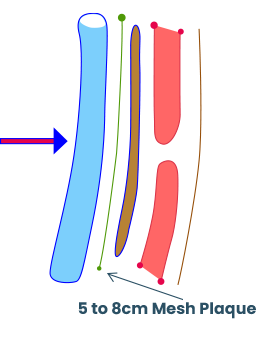
- Intestin pinched in the hernia
- Peritoneum lining
- Muscles separated by abdominal pressure
- Skin with hernia protrusion
After surgery
I- Open hernia surgery with mesh (tension free)
- The plate covers the inguinal region and is positioned ahead of the musculo-aponeurotic wall
- There is no tension at the muscular level
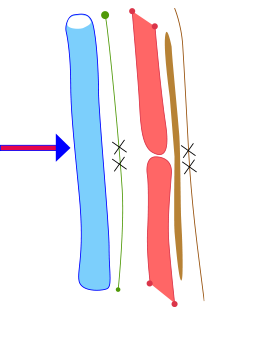
II- Open hernia surgery without mesh
X successive sutures
- skin
- muscles
- peritoneum
The wall is strenghtened with sutures alone
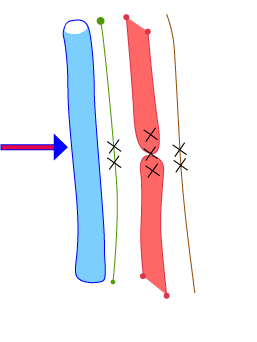
III- Laparoscopic hernia surgery
- The mesh plate largely covers the hernia and is pressed again the muscular wall
- There is no tension at the muscular level
WHITE LINE HERNIA / UMBILICAL HERNIA
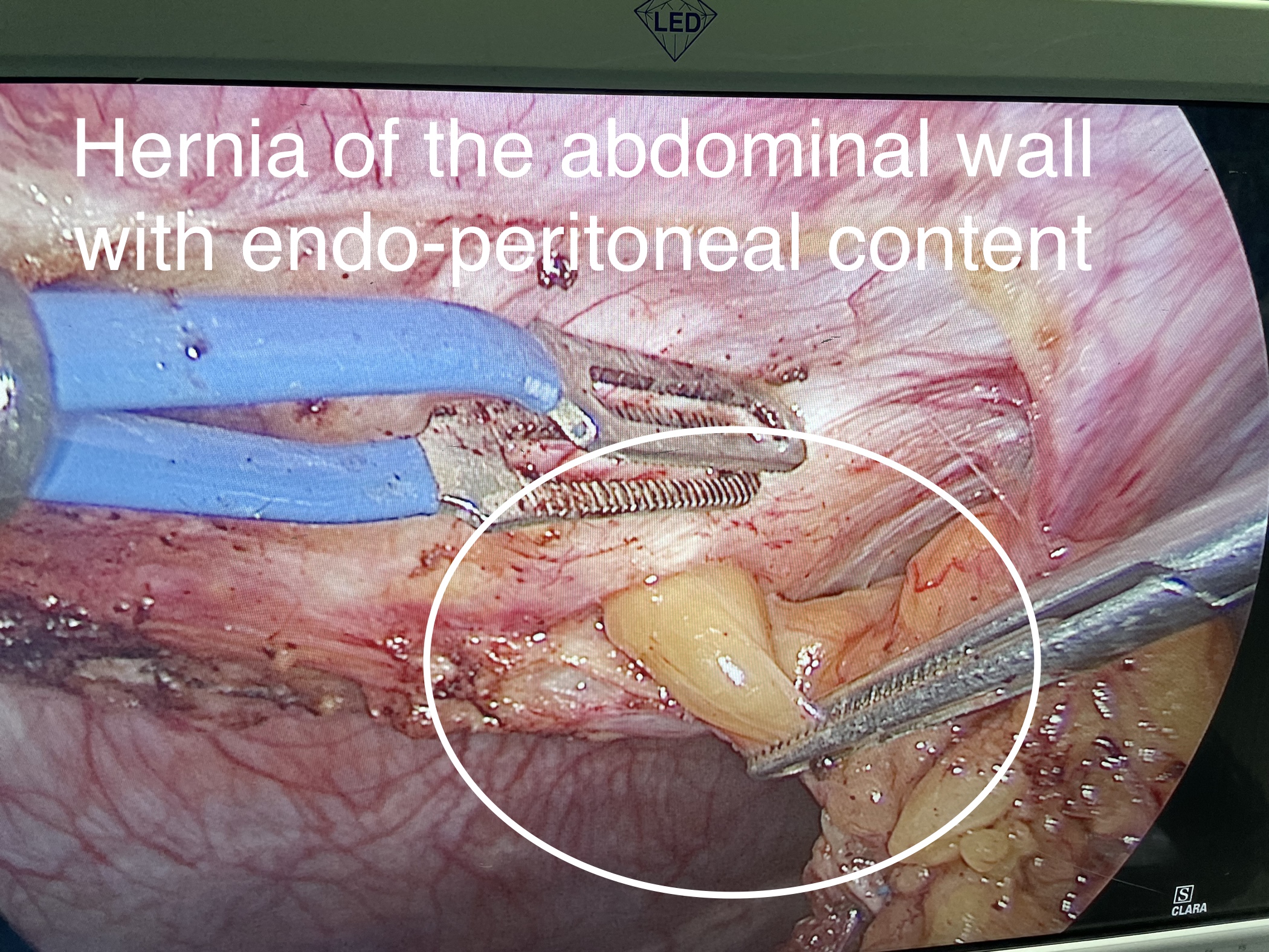
It is diagnosed when a “lump” appears in the midline of the abdomen, usually at or above the umbilicus, which may contain fat or intestine. This protrusion is more evident when standing or after physical exertion. It may contain fat (omentum, round ligament) or intestine.
Hernias can be divided into three categories:
Uncomplicated or reducible hernia: it is easily reduced under pressure or spontaneously when lying down.
Incarcerated hernia: it is blocked in the hernial orifice, but can still be reduced with the correct manual maneuvers.
Strangulated hernia: the hernia is very painful spontaneously, it is no longer reducible, immobile during coughing spells. The intense pain is due to the "suffering" of the hernial contents, which no longer receive adequate blood supply.
If it is not complicated, the hernia should be operated on only if it is associated with discomfort. Discomfort can manifest as pain, heaviness or simply psychological discomfort, which prevents us from performing the movements of our everyday life serenely.
The incarcerated hernia must be operated rather quickly, while the strangulated hernia constitutes a surgical emergency. In the latter case, a delay in treatment can lead to bowel resection as a complementary procedure to hernia repair.
Important: A hernia cannot improve over time, it can only deteriorate, although the rate of deterioration varies from patient to patient.
A linea alba or umbilical hernia may be associated with DIASTASIS (see Diastasis recti in the main menu) of the rectus abdominis muscles. In this case, the correction of the diastasis during the same procedure reduces the risk of a recurrence.
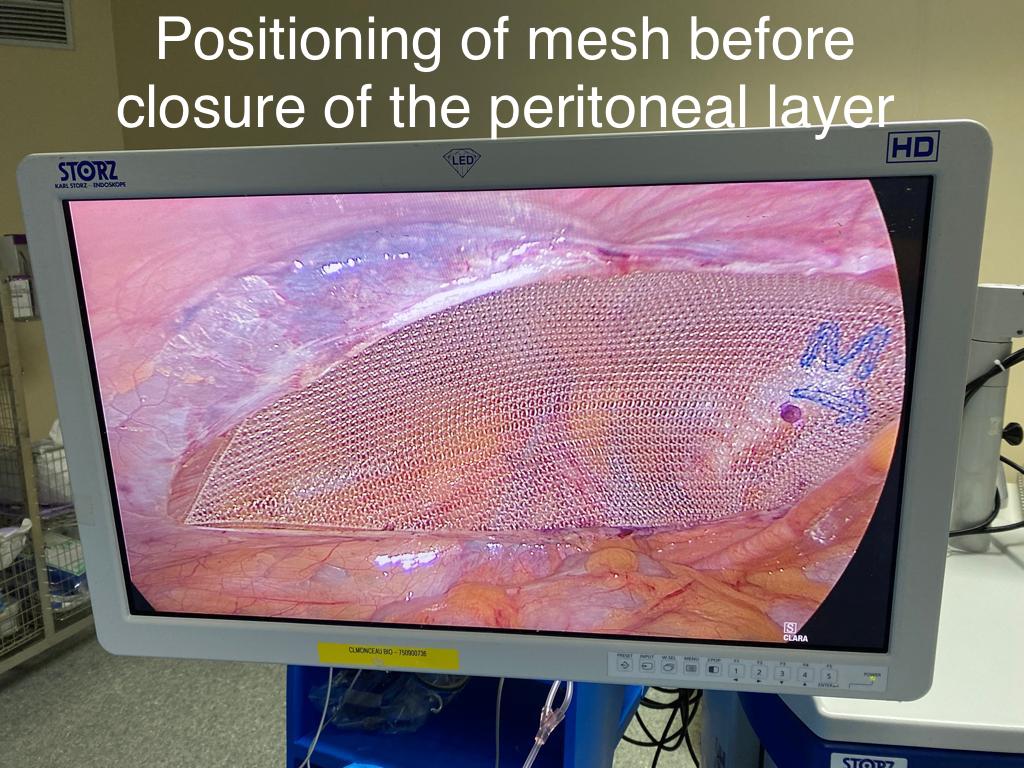
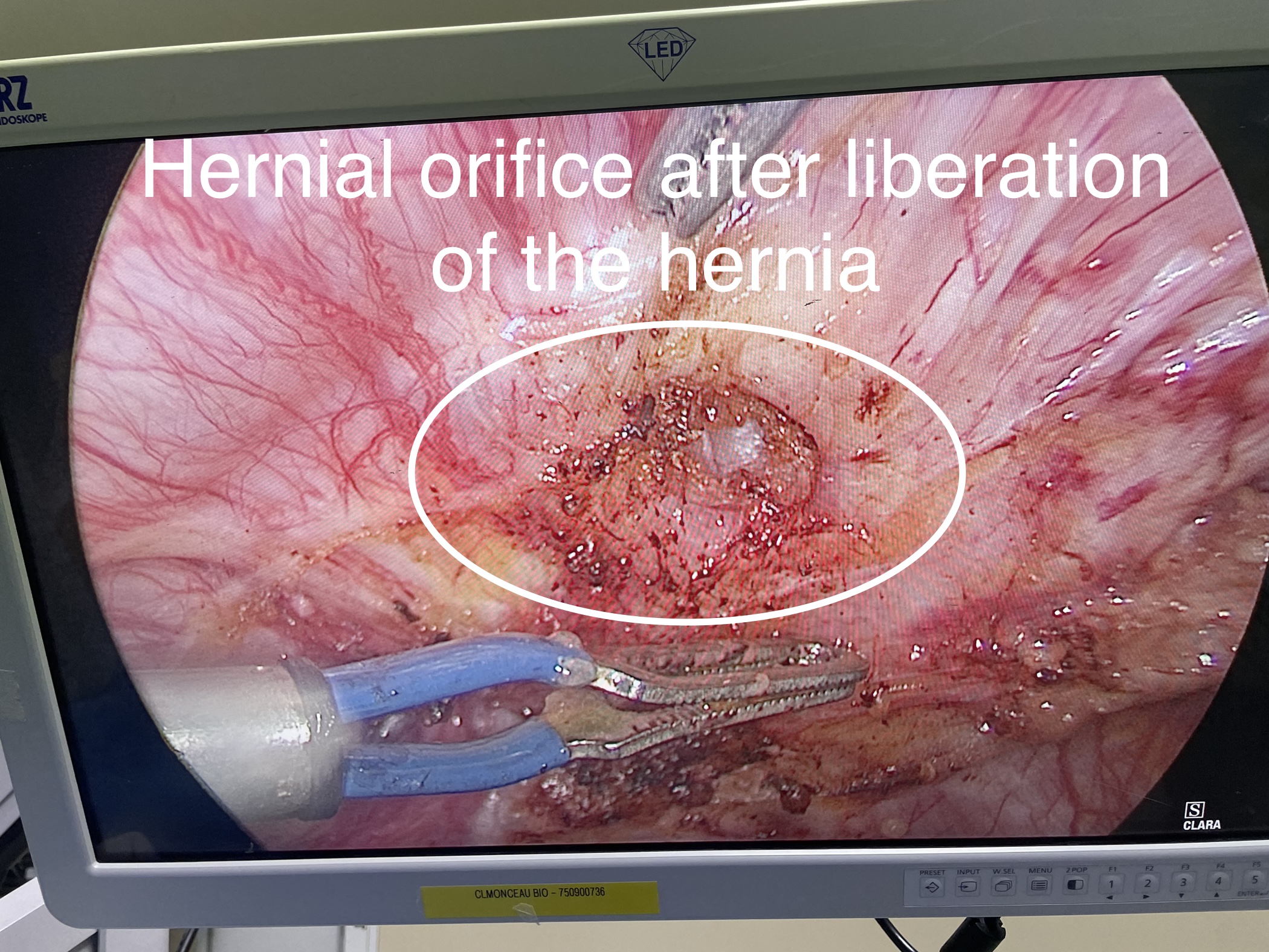
The treatment of umbilical or white line hernias consists of reducing the contents of the hernia in the abdomen and placing a mesh (prosthesis) which fills the parietal defect. If the net is placed behind the abdominal wall and intraperitoneally, the latter will be double-sided: an adherent side positioned facing the wall and a non-adherent side installed facing the abdominal cavity.
The approach can be by direct incision (laparotomy) or minimally invasive (laparoscopy) depending on the size and complexity of the hernia and/or the preferences of the surgeon. An advantage of the minimally invasive approach is the fact that the scars are located at a distance from the prosthesis; there will therefore be less risk of infection of the latter in the event of poor healing.
There is no particular diet after abdominal hernia repair surgery.
If the patient's profession does not involve too much physical effort, work can be resumed after about a week. For heavier jobs, it makes more sense to wait a month. In general, during the same period, it is better not to lift objects weighing more than 10 kilos.
During the first month, it is best to avoid constipation. You have to drink enough and eat plenty of fiber. You can also use a laxative to soften the stool.
Regarding physical exercise, although in general it is beneficial as it stimulates circulation, it will take about three weeks before resuming more intense physical activity such as sports. For the first three weeks one will be limited to carrying out simple daily tasks.
For more information on hernias:
Inguinale hernias (In French)
Umbilical hernias (In French)
Incisional hernias (In French)
Hernia and Diastasis Surgery can be performed on an outpatient basis.
Instagram: To see videos/reels regarding robotic hernia surgery performed by Dr. Randone click on the icon in the bar of your screen or here.
♦ Also see : INTERNATIONAL PATIENTS WELCOME
♦ To make an appointment with Dr. Bruto Randone, an ENGLISH SPEAKING Digestive Visceral and Abdominal Surgeon, at the Clinique Internationale du Parc Monceau, 21 Rue de Chazelles
, 75017 Paris, France, or at the Clinique Bizet, 23 Rue Georges Bizet, 75116 Paris, France, click on Contact.
• WhatsApp : https://wa.me/33769923387
